Anatomy Of The Adductor Magnus Muscle - Everything You Need To Know - Dr. Nabil Ebraheim
Dr. Ebraheim’s educational animated video describes the anatomy of the adductor magnus muscle.
Follow me on twitter:
https://twitter.com/#!/DrEbraheim_UTMC
Find me on Instagram @OrthoInitiative
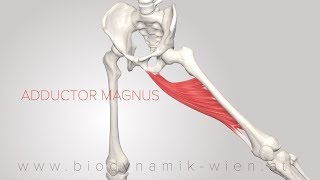
Anatomy of the Adductor Magnus Muscle
The adductor magnus is a very thick triangular muscle. There are two parts the pubic part and the ischial part. The pubic part arises from the inferior pubic ramis. The ischial part arises from the ischial ramis and the inferior lateral part of the ischial tuberosity. Ischial muscle part is the largest and thickest. The ischial part is close to the hamstring muscles, and it acts like the hamstrings. The pubic part inserts into the gluteal tuberosity, the Linea aspera, and the supracondylar ridge. Linea Aspera is a ridge of roughened surface on the posterior surface on the posterior surface of the femur. The ischial part (thick part) descends vertically and inserts into the adductor tubercle. The ischial part goes from the ischial tuberosity to the tubercle. The adductor magnus muscle is located within the medial compartment of the thigh. The adductor magnus muscle is innervated by obturator nerve and by the tibial part of the sciatic nerve. The pubic part is the adductor part supplied by the posterior division of the obturator nerve. The hamstrings part of the ischial part is supplied by the tibial nerve. From proximal to distal, the muscle is supplied by the obturator artery, the deep femoral artery, and its perforating branches, and from small muscular branches arising directly from the femoral artery. The pubic part is a true adductor of the thigh. The ischial part extends the hip. While in a sitting position, the examiner has the patient squeeze the thighs with resistance placed at the inside of the knees. Weak thigh adduction indicates obturator nerve injury. It is advised not to use a compression hip screw in the intertrochanteric reverse oblique fracture of the hip. Medial displacement of the distal fragment may occur due to the pull from the adductor muscles. Strong pull and displacement of the distal femur fracture fragment by the adductor muscle occurs in the subtrochanteric fractures. Adductor myodesis is a critical part of a transfemoral amputation. If it is not performed, the abductors and hip flexors can cause the femur to abduct, leading to severe problems with gait. Adductor myodesis improves the clinical outcome, provides soft tissue envelope that helps in prosthetic fitting, it improves position of the femur, and allows more efficient ambulation. The adductor magnus muscle is 4 times larger than the longus and brevis. Above knee amputation could result in 70% loss of the adduction moment. For maximum prosthetic control after distal transfemoral amputation, myodesis should be done, and the residual limb is maintained in slight adduction.