Approach to breast mass
This is a short video on the approach to a breast mass.
This presentation was made with Google Slides.
Images and figures were created or adapted from Wikimedia Commons.
ADDITIONAL TAGS:
Approach to a breast mass
Palpable breast mass
Age 30
Age =30
Mammogram
+/ ultrasound
Ultrasound
+/ mammogram
Complex: irregular/indistinct borders, thickwalled, heterogeneous mass, septated, solid and cystic components, calcifications
Smooth (homogeneous), mobile, thinwalled, anechoic (fluidfilled), no echogenic debris, wellcircumscribed → likely a simple cyst
Tissue sampling: Fine needle aspiration (minimally invasive)
for suspected cysts or small masses
Core needle biopsy for solid, acellular masses → ER, PR, Her2/neu receptor testing
Open (excisional) biopsy for large, suspicious masses → frozen section, sentinel node biopsy
Symptomatic
(pain, pressure)
Asymptomatic
Fine needle aspiration
Observation
Bloody aspirate
Nonbloody aspirate (clear, strawcolored, green, gray)
Cyst persists / recurs
Cyst resolves
Ultrasoundguided core needle biopsy, consider additional imaging
Done! Low risk for cancer
Age: adolescent AND mass is not concerning: solitary, firm, wellcircumscribed, mobile, cyclic premenstrual tenderness → likely a benign fibroadenoma. Observe and reeval in 6 weeks.
Increasing size
↓ in size, tenderness → Done!
+/ surgical resection (wide local excision vs lumpectomy vs total mastectomy +/ axillary lymph node dissection)
+/ chemo (ER+ or PR+ should get tamoxifen, raloxifene, or aromatase inhibitors [anastrozole, letrozole, exemestane]; Her2/neu+ get trastuzumab)
+/ radiation
Physical exam
Inspection → palpation
Signs concerning for cancer:
Invasion of lactiferous ducts → nipple retraction
Epidermal infiltration by neoplastic cells → scaling or ulceration
Invasion of suspensory (Cooper) ligaments → skin retraction
Obstruction of dermal lymphatics → peau d’orange
Invasion into adjacent breast tissue → fixed mass
Lymphatic spread to regional lymph nodes → axillary lymphadenopathy
History
HPI: SOCRATES (site, onset, character, radiation, associations, time course, exacerbating/relieving factors, severity)
Change in breast appearance (size, symmetry)
Single or multiple masses
Change in mass appearance
Skin changes
Nipple inversion
Discharge (uni/bilateral, timing, color)
Cyclic nature with menstrual cycles (fibroadenoma or fibrocystic changes?)
Tender or nontender
Fluctuant (abscess?)
Fixed or mobile
Recent trauma / surgery (fat necrosis?)
Risk factors:
Amount of estrogen exposure: older age, younger menarche, older menopause, use of OCPs, obesity, high bone density, low/no parity
Family history in first degree relative (mother or sister)
BRCA1/2 positive
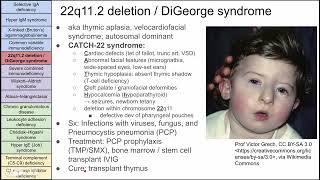
Approach to a breast mass: history and physical exam