
Can compression of the Spinal Cord affects the Hand Function?
Compression of the spinal cord and hand function
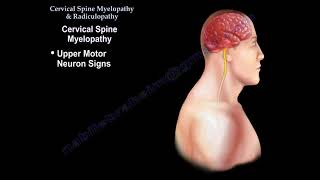
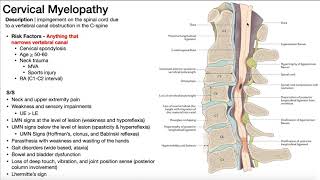
Cervical myelopathy is a form of neurologic impairment due to compression of the spinal cord in the cervical canal.
MRI is usually the study of choice to diagnose cervical myelopathy. The natural history of a cervical myelopathy is a
slow, stepwise deterioration over time with variable periods of stable neurologic function. Changes in hand
dexterity and coordination are among the earliest signs and these may be present in otherwise asymptomatic
individuals. The progressive cervical cord compression can result in intrinsic atrophy, weakness in grip and pinch,
small finger escape, and impaired ability to perform rapid alternating movement. Thorough history and physical
exam is important given the often asymptomatic, but progressive nature of cervical myelopathy. The lower cervical
nerve roots (C8T1) are most severely affected. The clinical presentation of cervical myelopathy is highly variable.
The typical patient with cervical myelopathy will complain of symmetric numbness and tingling in the extremities.
The diffuse numbness in the hands is often misdiagnosed as carpal tunnel syndrome. It requires a high index of
suspicion given the progress deterioration in patients with cervical myelopathy. About 20% of patients in the
myelopathy group do have myelopathy signs on physical exam. Myelopathic hand describes a patient with
myelopathy of the cervical spine and its associated findings in the hand. The patient will have hand clumsiness and
gait disturbance. The patient may have decreased manual dexterity. The patient will have difficulty manipulating
objects such as buttoning and on buttoning her shirt. Patient may be dropping objects, because they cannot hold it.
The patient is usually an older patient who may complain of occipital headache.
What is the myelopathic hand?
The patient will have difficulty with grip and release. The patient will have loss of motor strength, will have sensory
changes and intrinsic wasting. There will be a finger escape sign and spasticity. The patient will have difficulty with
hand dexterity, will have hyperreflexia, a positive Hoffmann sign, a positive Romberg sign and gait disturbance. The
patient will feel unstable on their feet.
What is the finger escape sign?
Asked the patient to hold the fingers extended and adducted. The small finger will spontaneously abduct due to
weakness of the intrinsic muscle. The ulnar 2 digits drift into abduction and flexion within 30 seconds is also
described.
Grip and release test
Normal patient will make a fist and release it 20 times in 10 seconds. A myelopathic patient will not be able to do
that. In a positive grip and release test, the patient has trouble making a fist and fully extending the fingers. There
will also be loss of coordination and dexterity of the hand during rapid movement.
Hoffmann sign
A positive Hoffmann sign occurs when snapping the patient's distal phalanx of the middle finger leads to
spontaneous flexion of the other fingers (most common physical exam findings).
Babinski test
The patient may have a positive Babinski test which is positive with extension of the great toe.
Clonus test
The patient may have sustained clonus (more than 3 beats).
The Hoffman sign is only reliable in about 60%, Babinski in about 13%, and clonus in about 13%. The condition is
usually progressive (gets worse with time) and it rarely improves without surgery. Surgical treatment will entail
decompression and stabilization of the cervical spine. Early diagnosis and treatment of this condition is important to
achieve a reasonable, good outcome.











![Cavernous Malformation [2020] Ginger Burden | EP 97](https://i.ytimg.com/vi/9EfiX8XbFs4/mqdefault.jpg)








