cervical myelopathy and cervical radiculopathy- Everything You Need To Know - Dr. Nabil Ebraheim
Dr. Ebraheim animated video illustrates spine concepts associated the cervical spine cervical spondylosis and cervical myelopathy also cervical radiculopathy .cervical spine animation. Cervical disc herniation and surgery is presented.
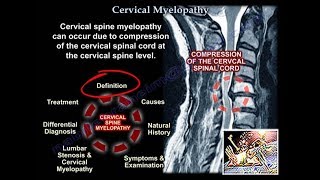
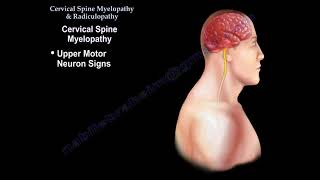
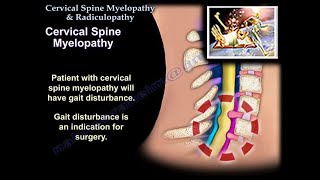
Cervical Myelopathy:
Patient will have gait disturbance, which is an indication for surgery.
Patient will also have upper motor neuron signs.
Upper extremity weakness.
If the hands are clumsy, you got myelopathy of the hands.
Xray will show spondylosis and loss of lordosis.
MRI will show compression of the cervical spinal cord.
Some of these patients will have lumbar spinal stenosis and they come to the doctor with an MRI and they have gait disturbance.
Check the C spine; get an MRI of the C spine.
The exam may be confusing because they may come to the doctor with low back pain and positive MRI for lumbar stenosis.
Ask about neck pain and stiffness, and if they feel unstable when they walk, and examine them for upper motor neuron signs:
Spasticity hyperreflexia
Hoffman’s sign: presence of this reflex indicates an upper motor neuron lesion due to cervical spinal cord compression.
Clonus
Babinski
Gait disturbance can occur in thoracic disc, which occurs in males, there will be pain with radicular symptoms, with normal upper extremity exam and there will be upper motor neuron findings in the lower extremity such as clonus and Babinski reflex.
If you are going to do surgery on cervical myelopathy, which approach will you use?
You will use anterior approach of the cervical spine especially when there is a kyphotic spinal segment.
Go anterior, especially if there is cervical spine kyphosis more than 10° because this can be corrected anteriorly.
The airway compromise occur when the surgery takes more than 5 hours in the upper cervical spine, occurring at more than three levels, and more than 300 ml of blood loss.
You may go posteriorly, laminectomy and posterior fusion, but kyphosis more than 10° is contraindication to going posteriorly.
Usually this operation is done for multilevel decompression.
Complications of the posterior approach:
Infection
If you do laminectomy alone, you will have progressive kyphosis.
C5 nerve root palsy may occur due to the anterior or posterior approach, it is unknown why it happens, the nerve recovers but it takes a long time to recover.
Cervical laminoplasty:
Is not used when there is fixed cervical spine kyphosis.
Somatosensory Evoked Potentials (SEPs)
Spinal cord monitoring technique
Positive if there is a 50% decrease in amplitude or a 10% increase in latency.
Recurrent Laryngeal nerve (RLN):
Vocal cord paralysis on one side will give hoarseness.
Superior Laryngeal Nerve (SLN):
Will affect the high note phonation, it can affect singers, there will be no vocal cord paralysis.
Usually occurs when dealing with upper cervical spine surgical approaches.
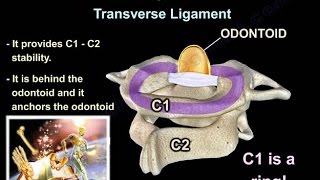
Where is the rotation of the C spine mostly occurring? In C1 and C2.
Flexion extension of the C spine mostly occur in C4 C5
Ankylosing Spondylitis:
HLAB27 positive
Chest expansion is less than 1 inch
Bamboo spine
May have occult fractures, especially cervical spine fractures; suspect it especially in patients with pain and negative xrays.
Need to get MRI or CT scan to see lt.
Need to admit this patient and have spine precautious because they may have neurological deficit most of the time due to epidural hematoma.
Xrays will show marginal syndesmophytes.
Need to recognize the difference between ankylosing spondylitis and diffuse idiopathic skeletal hyperostosis (DISH).
Involvement of the scaroiliac joint and the disc space favors ankylosing spondylitis.
When do you do the surgery and what kind of surgery?
You do spinal decompression and fusion
Usually long fusion especially if cervical spine is unstable, if there is progressive neurological deficit, or epidural hemorrhage.
Charcot of the Shoulder:
They will give you an xray of the proximal humerus that clearly disappeared, and they will ask you what are you going to do next?
You get an MRI of the spine to check for syrengomyelia of the cervical spine.
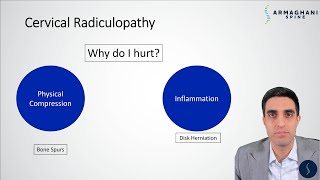
Cervical spine radiculopathy:
Pain and/or neurological symptoms resulting from conditions such as a disc herniation that irritates a nerve in the cervical spine.
Cervical spine and shoulder problems overlap, the patient’s symptoms are relieved by shoulder abduction and placing the hand over the head.
In cervical disc problems be aware of false positive MRIs.
It usually involves the lower numbered root, so if you have C6C7 you will get C7 nerve root compression.
Follow me on twitter:
https://twitter.com/#!/DrEbraheim_UTMC
Donate to the University of Toledo Foundation Department of Orthopaedic Surgery Endowed Chair Fund:
https://www.utfoundation.org/foundati...