Craniocervical 'tucking' a biomechanical fallacy and common cause of extracranial IJV stenosis

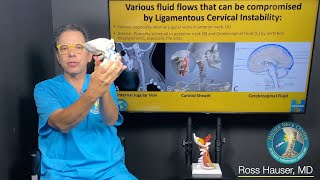
Biomechanical, extracranial stenosis of the internal jugular vein (IJV) is an increasingly commonly recognized problem (Larsen 2018c, Gweon 2011, Dashti 2012, Higgins 2015, 2017). It frequently occurs between the atlas and styloid process, and may occur as a sequela of forward atlantal subluxation (Larsen 2018c) as well as due to intermittent, positional obstruction (treningogrehab.no/atlas).
Continuous neck tucking will cause the styloid process to translate down and backwards, narrowing the atlantostyloid interval (ASI) which the neurovascular bundle (IJV + CN912) transmit through. Compression of these structures may cause intracranial hypertension, chronic fatigue, orthostatic disorders, vision impairment, audiovestibular disorders, and more (Jayaraman 2012, Higgins 2015, 2017, Larsen 2018c).
Thus we do NOT want to tuck the chin fully , and especially not in tandem with craniocervical extension as this may further narrow the ASI. We want to "elongate" the neck (Osar 2012, Larsen 2018c) without overly extending nor flexing the craniocervical junction (head), to maintain/promote a broad ASI.
Intracranial hypertension may often remain occult. It has been shown that many may have this problem despite normal lumbar punctures and cerebral MRI scans (Higgins 2015, 2017, Larsen 2018c). The subsequent chronic venous congestion may burden the dural membrane to such extent that it perforates, resulting in CSF leakage and intracranial HYPOtension. This may cause depression, severe fatigue, orthostatic headaches and tachycardia, etc.
Habitual cervical hinging and chin tucking is detrimental and should not be done.