ECG Quiz for ACLS and Clinical Practice

Homepage: EMNote.org ■
Membership: https://tinyurl.com/joinemnote
ACLS Lecture: https://tinyurl.com/emnoteacls
ECG Quiz for ACLS and Clinical Practice:
Case 1. The patient has digoxin overdose and presents with syncope.
The ECG shows bidirectional ventricular tachycardia.
Bidirectional VT is most commonly associated with severe digoxin toxicity.
Case 2. The patient presents with dizziness and shortness of breath.
The ECG shows second degree Mobitz type 2 AVblock.
Case 3. The patient presents with ischemic chest pain and diaphoresis.
The ECG shows posterior wall STEMI.
Case 4. The patient presents with chest pain on arrival and is asymptomatic during ECG.
The ECG shows Wellens syndrome, which indicates critical stenosis of the proximal LAD.
Stress tests are contraindicated in Wellens syndrome.
Case 5. The patient presents with ischemic chest pain and diaphoresis.
The ECG shows high Lateral STEMI caused by acute occlusion of the first diagonal branch of the LAD coronary artery.
This ECG pattern is called the South Africa Flag sign.
Case 6. The patient is a CKD patient presenting with general weakness.
The ECG shows tented peak T waves, due to hyperkalemia.
Case 7. The patient presents with ischemic chest pain and diaphoresis.
The ECG shows Anterolateral wall STEMI.
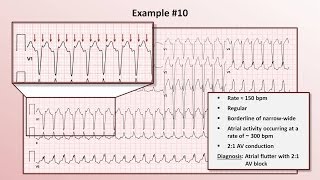
Case 8. The patient presents with palpitation and dizziness.
The ECG shows Atrial flutter with 3 to 1 AV conduction.
Case 9. The patient is a chronic alcoholic presenting with frequent syncope episodes.
The ECG shows torsades de pointes, which demonstrates a characteristic illusion of a twisting of the QRS complex around the isoelectric baseline.
It causes a sudden drop in arterial blood pressure, leading to dizziness and fainting.
Common causes include druginduced QT prolongation, low serum magnesium, low serum potassium, or congenital long QT syndrome.
Case 10. The patient presents with ischemic chest pain and diaphoresis.
The ECG shows Inferior wall STEMI.
Case 11. The patient has multiple myeloma and presents with an ECG with short QT interval.
The ECG is compatible with hypercalcemia: shortening of ST segment, shortening of QT interval, and presence of Osborn waves or J waves.
Case 12. The patient is an old lady with chronic atrial fibrillation presenting with nausea and vomiting.
Regularized atrial fibrillation and sagging of ST segments which resembles the “Salvador Dali’s moustache”, are ECG findings compatible with digitalis use.
Case 13. The patient is a young Asian male presenting with acute quadriparesis.
The ECG shows prolonged QT intervals.
The combinition of prolonged QT intervals and quadriparesis in Asian males suggests the diagnosis of toxic periodic paralysis which consists of hypokalemia and thyrotoxicosis.
Case 14. The patient is a CKD patient presenting with general weakness.
The ECG shows a sine wave pattern which is compatible with severe hyperkalemia.
Case 15. The patient is a homeless man found coma outdoor in a winter night.
The ECG shows bradycardia with Osborn waves or J waves, diagnostic of hypothermia.
Case 16. The patient is an ICU patient with septic shock and unstable hemodynamics.
The ECG shows a domeandspike ECG pattern called "spiked helmet sign", an ECG marker of high mortality risk, which has been most often noted in critically ill patients with mechanical ventilation.
Case 17. The patient presents with syncope and palpitation.
The ECG shows wide irregular rhythm, with heart rates approaching 300 per minute in some places, compatible with atrial fibrillation in preexcitation, such as WPW syndrome.
The drug indicated to treat stable patient with atrial fibrillation in WPW syndrome is procainamide.
Case 18. The patient is an Asian male presenting with syncope.
He has a family history of sudden death of his father at age 43.
The ECG shows Brugada syndrome.
Case 19. The patient is a young man with major depression, presenting with drug overdose and seizures.
The ECG shows several findings compatible with TCA intoxication, which include:
QRS above 100 milliseconds, sinus tachycardia, terminal R wave greater than 3 millimeters in aVR, and dominant Rprime in aVR.
Case 20. The patient presents with progressive dyspnea and enlarged cardiac silhouette on Chest XRay.
The ECG shows electrical alternans, an alternating QRS amplitude rhythm that is typically associated with the “swinging heart” surrounded by a large pericardial effusion.
Case 21. The patient is a young man presenting with upper respiratory tract infection, fever, and atypical chest pain.
The ECG shows diffuse PR depressions and ST elevations in multiple leads except lead aVR, which is compatible with acute pericarditis.
Spodick sign refers to downsloping TP segments found in acute pericarditis.
Case 22. The patient is a 56yearold man with acute dyspnea and chest discomfort.
The ECG shows sinus tahycardia, an S wave in lead 1, Q wave and an inverted T wave in lead 3.
"S1Q3T3" is suggestive of acute pulmonary embolism.