Examining a Person with Catatonia (Bush-Francis Catatonia Rating Scale)

Examining a Person with Catatonia (BushFrancis Catatonia Rating Scale)
Catatonia is a neuropsychiatric syndrome in which the cluster of behavioral, psychomotor, affective and cognitive symptoms secondary to medical, neurological, psychiatric and idiopathic reasons. In DSM5, catatonia is recognized as due to a medical or psychiatric condition, or unspecified, as, for example, in recurrent idiopathic catatonia. Mood disorders such as MDD and bipolar disorder are now recognized as more commonly associated with catatonia. These etiologies range from primary psychiatric disorders to general medical and neurological disorders, and drugs and substances of abuse.
The differential diagnosis of catatonia is extensive. Many conditions present with movement dysregulation and stupor. It is vital to perform a comprehensive medical examination and detailed neurological evaluation upon first contact with the patient. This should be accompanied by blood work, including a complete metabolic panel, blood count and analysis, electrolyte, kidney and liver function tests, a toxicology screen, as well as a battery of common hormonal values. A brain MRI and an electroencephalogram (to rule out nonconvulsive status epilepticus) are required. Some cases with fever or elevated neutrophil count will require examination of cerebrospinal fluid.
The common pathophysiology of catatonia entails a dysregulation of specific neural pathways affecting motor function and emotional regulation that relate to circuitry linking the medial frontal and inferior orbital cortices to the basal ganglia and thalami, with connections to the parietal lobes,
cerebellum, and limbic system. Thus, catatonia would be mediated by hypofunction of cortical (frontal) Gammaaminobutyric AcidA (GABAA) neurotransmission, leading to hypoactivity of subcortical dopaminergic pathways in the basal ganglia, VMPFC, DLPRC and Orbitofrontal cortex. In addition, glutamate has also been implicated in the pathophysiology of catatonia, being a biological antagonist of GABA, and because glutamate
antagonists improve catatonia.
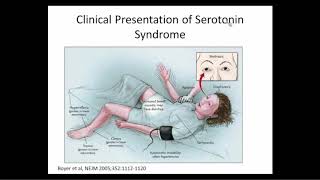
Differential diagnosis: Neuroleptic Malignant Syndrome is a medical emergency. It can lead to death if not treated. Patients with NMS typically present with fever, muscle rigidity and altered mental status. In some cases, akathisia, is sometimes seen rather that rigidity. Patients may develop delirium and mutism during the course of NMS and can appear much like cases of idiopathic catatonia. White blood cell count and CPK often increase in NMS and rhabdomyolysis is frequently seen. Hypertensive crisis and metabolic acidosis are common. Most patients will need the support of an intensive care unit to provide for adequate hydration, ventilation, and temperature regulation. Before doctor you try lorazepam challenge ascertain the functional nature by excluding all possible organic causes.
Only in the presence of normal laboratory values (all investigations should have been done and organicity should have been ruled out), a lorazepam challenge test can provide a confirmatory diagnosis. Most cases of catatonia will respond to 2–4 mg of intravenous lorazepam. The injection will usually bring about normal motor activity and restore mental clarity within one to two min. This reduction in symptoms is brief, lasting 20–30 min before the patient gradually returns to a rigid stupor.
The first order of care for the individual with catatonia is to establish the medical etiology. Along with the aggressively searching for the cause supportive treatment should be started immediately. The supportive care of the patient includes adequate hydration and other supportive measures. Concurrent care may include nutrition, cooling, prevention of aspiration, and consideration of thrombophlebitis prophylaxis. Once these measures have been taken, treatment of any underlying conditions should alleviate the psychomotor symptoms. This approach, however, does not manage all cases as catatonia may be idiopathic. Once medically stable, the active treatment usually falls into two categories, benzodiazepine activation or electroconvulsive therapy