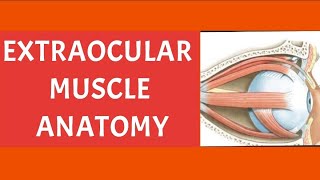
Extraocular Muscles | Location | Attachments | Nerve supply | Axes of muscles u0026 movements | Squint

TYPES OF EXTRAOCULAR MUSCLES
Voluntary Muscles 1. Four recti:
a. Superior rectus. b. Inferior rectus. c. Medial rectus. d. Lateral rectus. 2. Two obliqui:
a. Superior oblique.
b. Inferior oblique.
3 The levator palpebrae superioris elevates the upper eyelid.
Voluntary Muscles
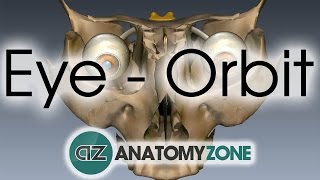
Origin
1. The four recti arise from a common annular tendon of tendinous ring of zinn.
The ring is attached to the middle part of superior orbital fissure.
The lateral rectus has an additional small tendinous head which arises from the orbital surface of the greater wing of the sphenoid bone lateral to the tendinous ring.
Through the gap between the two heads abducent nerve passes.
2. The superior oblique arises from the undersurface of lesser wing of the sphenoid, superomedial to the optic canal. 3. The inferior oblique arises from the orbital surface of
the maxilla, lateral to the lacrimal groove. The muscle
is situated near the anterior margin of the orbit.
4. The levator palpebrae superioris arises from the orbital surface of the lesser wing of the sphenoid bone, anterosuperior to the optic canal and to the origin of the superior rectus.
Insertion
1.The recti are inserted into the sclera, a little posterior
to the limbus (corneoscleral junction).
The average distances of the insertions from the cornea are: superior 7.7 mm; inferior 6.5 mm, medial 5.5 mm;
lateral 6.9 mm.
2. The tendon of the superior oblique passes through a fibrocartilaginous pulley attached to the trochlear fossa of the frontal bone.
The tendon then passes laterally, downwards and backward below the superior rectus.
It is inserted into the sclera behind the equator of the eyeball, between the superior rectus and the lateral rectus.
3. The inferior oblique is fleshy throughout.
It passes laterally, upwards and backwards below the inferior rectus and then deep to the lateral rectus.
The inferior oblique is inserted close to the superior oblique a little below and posterior to the latter.
4. The flat tendon of the levator splits into a superior or voluntary and an inferior or involuntary lamellae.
The superior lamella of the levator is inserted into the anterior surface of the superior tarsus, and into the skin of the upper eyelid.
The inferior lamella (smooth part) is inserted into the upper margin of the superior tarsus and into superior conjunctival fornix.
Nerve Supply
1. The superior oblique is supplied by the IV cranial or trochlear nerve (SO4).
2 The lateral rectus is supplied by the VI cranial or abducent nerve (LR6).
3 The remaining five extraocular muscles; superior, inferior and medial recti; inferior oblique and part of levator palpebrae superioris are all supplied by the III cranial or oculomotor nerve
Actions
1. The movements of the eyeball are as follows. a. Around a transverse axis . (Y axis) Upward rotation or elevation (33').
Downwards rotation or depression (33’).
b. Around a vertical axis . (X axis)
Medial rotation or adduction (50").
Lateral rotation or abduction (50').
c. Around an anteroposterior axis (Z axis) Intortion
Extortion.
The rotatory movements of the eyeball upwards, downwards, medially or laterally, are defined in terms of the direction of movement of the centre of the pupil.
The tortions are defined in terms of the direction of movement of the upper margin of the pupil at 12 o'clock position.
d. The movements given above can take place in various combinations.
Single or pure movements are produced by combined actions of muscles.
Similar actions get added together, while opposing actions cancel each other enabling pure movements. a. Upward rotation or elevation: By the superior rectus and the inferior oblique.
b. Downward rotation or depression: By the inferior rectus and the superior oblique.
c. Medial rotation or adduction; By the medial rectus, the superior rectus and the inferior rectus.
d. Lateral rotation or abduction: By the lateral rectus, the superior oblique and the inferior oblique. e. Intortion: By the superior oblique and the superior rectus.
f . Extortion: By the inferior oblique and the inferior rectus.
Combined movements of the eyes
Normally, movements of the two eyes are harmoniously coordinated.
Such coordinated movements of both eyes are called conjugate ocular movements
Clinical Anatomy
1. Weakness or paralysis of a muscle causes squint or strabismus,
which maybe concomitant or paralytic. Concomitant squint is congenital;
there is no limitation of movement, and no diplopia In paralytic squint, movements are limited, diplopia and vertigo are present, head is turned
in the direction of the function of paralysed muscle, and there is a false orientation of the field of vision.
Nystagmus is characterized by involuntary, rhythmical oscillatory movements of the eyes.
This is due to incoordination of the ocular muscles. It may be either vestibular or cerebellar/ or even congenital.
Follow me in blogspot https://humananatomylessons.blogspot... Follow me in blogspot https://humananatomylessons.blogspot...