Gut Malrotation Nonrotation and Volvulus for USMLE
Gut Malrotation, Nonrotation, and Volvulus is arrest of the normal gut as it rotates around the super mesenteric artery. Embryology, Signs and Symptoms, Diagnosis and Treatment for students taking USMLE Step 2.
EMBRYOLOGY
Normal at 6 weeks the gut goes through the yolk sac and as time goes on it continues to enlarge and goes into the yolk sac even further. At 9 weeks there is rotation of the gut and the distal part of the gut rotates until it is anterior to the proximal part of the gut. Afterwards the gut returns to the fetus abdomin and there is another 180 degree rotation continues. Therefore there is a total of 270 degree of rotation around the Superior mesenteric artery. There are two types of malrotation. The first type of gut malrotation is gut nonrotation and gut malrotation.
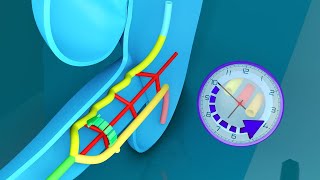
In gut nonrotation the the colon is on the left side of the small bowel. In gut malrotation, rotation does occur for a little bit but becomes arrested when on the way and therefore there is no downward movement. Gut malrotation is associated with more clinical findings due to the mesentary. The mesenteric base is really small and normally it goes from the duodenojejunal flexure down to the cecum. However, in gut malrotation it is much easier for it to spin on itself and this is known as volvulus. There is also formation of Ladd Bands which goes over the dudoenum and causes obstruction of dodenum.
Sign and symptoms of gut malrotation is related to the narrow mesentery allowing volvulus to occur which can lead to ischemia and necrosis. Ladd bands will cause duodenal obstruction.
Presentation of gut malrotation starts in infancy with biluous vomiting. There is also abdominal pain and distention. If volvulus occurs there may be some associated bloody stool which is a poor sign because it suggests ischemia and necrosis of the gut. This may lead to sepsis and fluid third spacing and therefore you must maintain fluid levels. Volvulos ocurs in about 22% in children and 12% in adults. There are a few differential diagnosis. Age is the biggest factor. In the preterm group there is necrotizing enterocolitis and this can differentiated by xray. In older infants there may be intussesception which is telescoping of the small intestine, which can be done through ultrasound bulls eye sign.
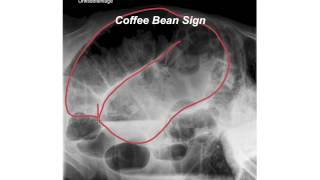
On Xray there will be gas and double bubble sign due to dudodenal obstruction from Ladd bands blocking dudodenum. Barium swallow or Gi series which is highlight the walls of the very nicely. In Volvulus there will be a classical corkscrew appearance. Often times there will be a misplaced dudonum which can be highlighted as well. Another imaging modality you can use Barium Enema, which will highlight the colon. The cecum is present on the right side of the abdomen. In a patient with gut nonrotation the cecm is on the left side of the large bowel. An ultrasound can also be performed and will show abnormal placement of the duodenum, Superior mesenteric Artery and Superior Mesenteric Vein. In volvulus there will be a classic whirpool sign.A CT scan is not perferred in children and adolescent, but in adults it can show perforation. Same findings on CT scan that are normally seen on Ultrasound. If findings are still equivocal than a laparatomy may be performed.
TREATMENT is primarily a surgical procedure known as the Ladd Procedure. The bowel is not returned to the normal position. The mesenteric base is widened, the Ladd Bands are removed and appendix is removed Adverse effects of Ladd Procedure may be short bowel syndrome can no longer absorb enough nutrients required. It may also leads to adhesions which may lead to intestinal obstruction. Prognosis is good because 89% will resolve. Mortality rate is zero with normal infants, but a slightly higher risk of mortality if there are other features.