Hypernatremia for USMLE Step 2
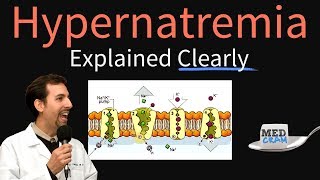
Hypernatremia is defined as a serum sodium concentration of greater than 145 mmol/L. By definition this is also known as a hyperosmolar state.
PHYSIOLOGY of SODIUM
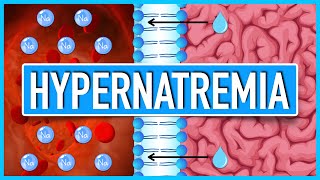
There are three spaces known as the intravascular, interstitial and intracellular space. Fluid is distributed throughout this entire area. The fluid present in the intravascular and interstitial space is known as the extracellular fluid (ECF). Within this area the fluid freely moves and there is not affect on changes electrolyte concentration. The intracellular fluid is twice the volume of extracellular space.
The movement of water is always towards the direction of the highest solute. In the intravascular space, the sodium has the strongest affect on water to move water towards the vascular space. So high sodium will cause increase water in the intravascular space, while low sodium decreases the amount of sodium in the intravascular space. Glucose and urea also have the same effect. Therefore the plasma osmolality is determined by 2xNa+Glucose/18+BUN/2.8 which is normally between 270290. BUN is known as the ineffective osmole because it can move freely into the cell and therefore it can't push water in any direction. The tonicity is the same as plasma osmolality except BUN is not taken into the consideration.
PATHOPHYSIOLOGY OF HYPERNATREMIA
Either due to loss of total body water or increase in sodium. Normally osmoreceptors in hypothalamus get activated (280290 mosmol/L). This leads to increasing thirst and ADH.
Regulation of brain volume is important to consider with looking at the pathology. During hypernatremia, acutely the neuron will lose water and lead to dehydration. After some time electrolytes move into cell and the water follows leading to partial restoration. Chronically (after 2 days) there is movement of oraganic osmolytes (AA, polyol, mehtylamine) and this can cause the brain cell to return to normal size.
ETIOLOGY AND CAUSES OF HYPERNATREMIA
Hypovolemic hypernatremia occurs when there is loss of water and sodium. Nonrenal causes will have urine sodium less than 10. This is most commonly associated with sweating, osmotic diarrhea, decreased water drinking and thirst, which is most common cause of hypernatremia in elderly and debilitated. In these patients the urine osmolality is greater than 800. Pancreatitis, burns and trauma may also cause these. Renal causes will have a urine sodium greater than 10 caused by excessive diuretic use (mannitol), adipsic diabetes insipidus, septor optic dysplasia, brain tumor.
Hypervolemic hypernatremia occurs when there is sodium retention. Non renal the FeNa is greater than 2%. Iatrogenic causes associated with sodium bicarbonate during metabolic acidosis. Hydatid cyst treatment, abortion and salt poisoning may lead to hypernatremia. Renal causes has a FeNa less than1% and caues by hyperaldosteronism.
Euvolemia is loss of sodium without water. Common causes is diabetes inspidus and hypothyroidism.
CLINICAL SIGNS AND SYMPTOMS of hypernatremia
Acute is less than 48 hours. There is rapid decrease in rapid decrease in brain volume leading to rupture of cerebral veins and demyelinating brain lesions. Symptoms initially present as lethargy, weakness, irritability, obtundation, decrease level of concsiousness, seizure, coma and eventual death.
Chronic is defined as hypernatremia lasting longer than 48 hours. Since it is occuring more slowly the brain is able to adapt to these changes.
INVESTIGATIONS for hypernatremia.
Serum electrolytes and osmolarity, glucose, urea, creatine and ADH.
Urine electrolytes, omsolarity, urine volume over 24 hours.
CT/MRI is important if considering Diabetes Insipidus.
TREATMENT of hypernatremia
3ml H20/kg will decrease sodium 1meq/L
Chronic hypernatremia should be correct slowly because the brain has adjusted to the change in sodium and may lead to brain edema. Decrease serum sodium less than 10meq/day. Any faster than this speed may lead to cerebral edema. IV destrose 5% water at a rate of 1.35/ml/hr/kg and monitor every 46 hours.
Acute hypernatremia requires rapid adjustment and so need to prevent any neurological damage. Generally reach normal sodium wihtin 24 hours. IV Dextrose 5% water 3 6ml/hr/kg and monitor every 1 to 2 hours until sodium is below 145 meq/L. Then give 12meq/L/hr until restored.
Water defecit is calculated by TBW x (serumNa/140 1). TBW is generally 60/55% in young adult and 50/45% in elderly and even less if obese. Replace ongoing water loss such as sweat and stool (3050ml/hr) and urine.