Ligaments of the Elbow Stability Of The Elbow - Everything You Need To Know - Dr. Nabil Ebraheim
Dr. Ebraheim’s educational animated video describes ligaments of the elbow and stability of the elbow.
Follow me on twitter:
https://twitter.com/#!/DrEbraheim_UTMC
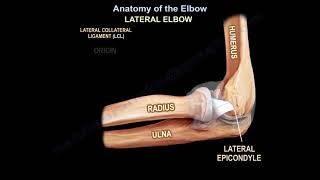
The primary stabilizer of the elbow is the ulnohumeral joint. The coronoid process is the anterior buttress of the olecranon. The coronoid process prevents posterior dislocation of the elbow. Fractures of the coronoid more than 50% of the height will lead to elbow instability. With fracture of the coronoid process, it is important to recognize the anteromedial fracture. LCL tear and impaction fracture of the anteromedial coronoid facet will lead to posteromedial instability of the elbow joint. Sometimes this fracture is not easily seen on the xrays and it can be missed. Delayed treatment of this fracture may result in varus and posteromedial instability, and early onset of osteoarthritis. Surgical fixation should be done and usually done through a medial approach. Posteromedial instability results from a varus deforming force. The coronoid process is also the attachment site for the important ligament, the anterior bundle of the medial collateral ligament of the elbow. Fracture of the coronoid process can also be a part of the terrible elbow triad. The MCL is composed of three bands, the anterior, posterior, and transverse bundles. The anterior band of the MCL is the strongest primary stabilizer to valgus stress in 90 degrees of flexion. In extension, it provides about 30% of the restraint. The osseous and articular components of the elbow joint, as well as the anterior joint capsule, resist the valgus forces in extension. The MCL originates from the posterior medial epicondyle of the distal humerus. It inserts into the sublime tubercle of the medial coronoid process. Late cooking and early acceleration will give the highest valgus torque to the medial collateral ligament. The deficiency of this ligament is diagnosed with the moving valgus stress test or the valgus stress test. With the arm fully supinated, find the MCL and take the forearm, placing a valgus stress on the medial collateral ligament. The elbow valgus stress test is used to assess the integrity of the medial collateral ligament. Clinical exam is not as good as the MRI. MRI is the best study to diagnose complete tears of the MCL of the elbow. CT scan arthrogram is more sensitive than MRI for partial lesions. In case of complete tear, reconstruction of the medial collateral ligament (ulnar) deficiency is the best procedure. Indication for surgery would be a complete tear in high level throwing athletes. 90% return to preinjury level of activity. The posterior portion of the MCL forms the floor of the cubital tunnel. The posterior bundle of the MCL is tight in elbow flexion. If you want to get more flexion of the stiff elbow, release the contracted posterior band of the medial collateral ligament. The third part of the MCL is called the transverse bundle. The LCL complex consists of four parts: lateral ulnar collateral ligament (LUCL), lateral radial collateral ligament (RCL), accessory lateral collateral ligament (ALCL), and annular ligament (AL). The lateral ulnar collateral ligament (LUCL) is the key anatomic structure which prevents posterolateral instability. The radial collateral ligament (RCL) and the accessory collateral ligament (ALCL) has some contribution to lateral elbow stability. All of this is debated and controversial, but there is consensus that the lateral collateral ligament complex and not an individual ligament is important in preventing posterolateral rotary instability of the elbow. The lateral ulnar collateral ligament (LUCL) acts like a sling for the radial head. The LUCL traverses the posterolateral aspect of the radial head. The LUCL originates from the lateral humeral epicondyle. The LUCL inserts into the crista supinatoris of the proximal ulna. Posterolateral rotary instability of the elbow occurs with LUCL deficiency. It is diagnosed with a lateral pivot shift test. The LUCL is deep and slightly distal to the common extensor tendon. Surgical approaches and arthrotomy to the lateral elbow may damage the ligament and may result in posterolateral instability of the elbow. Posterolateral rotary instability can also occur from iatrogenic injury to the LCL during treatment of tennis elbow. This can be a complication of surgery or can be part of the pathology that involves the extensor carpi radialis brevis muscle. It may also occur from injection of steroids into this area. This ligament that is close to the tendon can be injured due to excessive release of the origin of the ECRB tendon. The patient will have a painful click and difficulty achieving a full elbow extension after surgery. To avoid this condition, keep the detachment of the tendon anterior to the equator of the radial head. The annular ligament stabilizes the radioulnar joint. The radial head is important and provides approximately 30% of valgus stability.