Tarsal Tunnel Syndrome - Everything You Need To Know - Dr. Nabil Ebraheim
Dr. Ebraheim’s educational animated video describes tarsal tunnel syndrome medial ankle.
The tarsal tunnel is a fibroosseous tunnel posterior and inferior to the medial malleolus. The tunnel is covered by the flexor retinaculum, which protects the structures contained within the tunnel. The flexor retinaculum is a thick ligament that runs between the medial malleolus and the calcaneus.
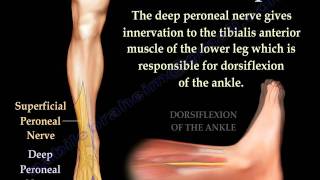
The structures which pass through the tunnel include the Tibialis posterior, the flexor Digitorum longus, posterior tibial artery, the tibial Nerve, and the flexor Hallucis longus. We are interested in the tibial nerve which lies between the posterior tibial artery and the flexor Hallucis longus.
Tarsal tunnel syndrome is a compression neuropathy caused by compression of the posterior tibial nerve within the tarsal tunnel. Tarsal tunnel syndrome is the most common compression neuropathy in the ankle and foot. Thickening of the flexor retinaculum may cause compression of the posterior tibial nerve.
Causes
80% of the cases are associated with a specific cause.
•Spaceoccupying lesion as lipoma or ganglia
•Varicose veins
•Muscle anomalies
•History of trauma
•Tenosynovitis
•Rheumatoid arthritis
•Diabetes
•Malaligned foot.
Symptoms of tarsal tunnel syndrome include burning pain, numbness, tingling, electric shock sensation typically around ankle or at the bottom of the foot (plantar aspect of the foot). Symptoms are worse with activity such as walking, standing or running. Tarsal tunnel symptoms are relieved with rest and elevation. Pain associated with tarsal tunnel syndrome may be worse at night. There may be swelling around the ankle and the foot.
Patient will have a positive compression test and a positive tinel’s sign. Tapping on the nerve posterior to the medial malleolus causes radiating pain into the medial side of the ankle and possibly to the foot.
Pressure within the tarsal tunnel increases with ankle dorsiflexion and foot eversion. This may reproduce the symptoms. Pain associated with tarsal tunnel syndrome radiates proximally and distally.
Tarsal tunnel may present as part of the heel pain triad which occurs in adults. The heel pain triad includes tarsal tunnel syndrome, plantar fasciitis and acquired flat foot deformity.
Diagnosis is by combination of history, examination, EMG and nerve studies that can lead you to the diagnosis (history is the most useful examination, EMG is accurate in about 8090%). The dorsiflexioneversion test is described to be helpful in the diagnosis of tarsal tunnel. Sensory nerve conduction studies are more helpful than motor studies (EMG). Always rule out radiculopathy.
Radiographs and CT scan may show osseous impingement or posteromedial process fracture of the talus. MRI may show a space occupying lesion such as a ganglion cyst or lipoma.
Differential diagnosis includes Peripheral neuropathy that involves all the nerves, not just the tibial nerve. Sural nerve and saphenous nerve are also involved and there will be an absent ankle jerk.
Treatment is immobilization, antiinflammatory medications, and steroid injections. Patient may have orthotic with medial posting if the patient has a valgus hindfoot.
Surgical release of the tarsal tunnel if nonoperative treatments fails after a trail of 36 months.
•Release the fascia proximal to the flexor retinaculum.
•Release the flexor retinaculum.
•Identify the tibial nerve proximal to the tunnel and decompress the nerve and its three branches.
•Decompress the entire tunnel 5 cm proximal to the flexor retinaculum and distally to the deep fascia of the abductor hallucis.
•Distal release of the Baxter’s nerve is usually done if the patient has chronic plantar medial heel pain (heel pain is uncommon in tarsal tunnel).
•Decompress the Baxter’s nerve by release of the deep fascia of the abductor hallucis.
•Remove any space occupying mass.
Best results occur if symptoms occurred in less than one year. A successful outcome occurs in about 5090% of the cases. The best result occurs if the patient has space occupying lesion with a positive physical examination and EMG findings. The suboptimal results can occur from inadequate release traction neuritis and repeat tarsal tunnel release. In these situations, the patient will not respond well to surgery (always rule out double crush syndrome).
Revision surgery has a less successful outcome unless the patient has an inadequate release.
Recurrence of tarsal tunnel syndrome is usually caused by inadequate release and repeat tarsal tunnel release is usually not advisable. In general, tarsal tunnel decompression may not produce a good longterm outcome.
Become a friend on facebook:
/ drebraheim
Follow me on twitter:
https://twitter.com/#!/DrEbraheim_UTMC












![Inside of the Ankle Pain [Tarsal Tunnel Syndrome Treatment & Symptoms]](https://i.ytimg.com/vi/gYHSsc6yW68/mqdefault.jpg)