The Superior Gluteal Artery - Everything You Need To Know - Dr. Nabil Ebraheim
Dr. Ebraheim’s educational animated video teaches about the Superior Gluteal Artery, and describes its function and where it supplies, and what are the common injuries affecting this artery, also provides you with a simple images that helps you understand more.
The superior gluteal artery is an important artery; injury to it may cause excessive bleeding.
The aorta bifurcates at the level of L4 forming into 2 iliac arteries, which is about 4cm long and ends in front of the SI joint, and each common iliac artery divides into external and internal iliac arteries.
The internal iliac artery is the major arterial supply of the pelvis.
The internal iliac artery divides into2 parts: anterior and posterior division.
The superior gluteal artery is a branch of the posterior division of the internal iliac artery, it reaches the gluteal region through the greater sciatic notch above the periformis, it divides into superficial and deep branches.
The superficial division enters between the gluteus maximus and medius, so it enters the deep surface of the gluteus maximus.
The deep division passes between the gluteus medius and the gluteus minimus; it lies on the deep surface of the gluteus medius.
The inferior gluteal artery is a branch of the anterior division of the internal iliac artery; it leaves the pelvic through the greater sciatic notch below the periformis muscle.
It supplies the gluteus maximus and also gives the following branches:
1 The sciatic artery: the vasa nervosa, it runs with the sciatic nerve.
2 Anastomotic branch: joins the cruciate anastomosis.
So the superior gluteal artery is above the periformis muscle, the inferior gluteal artery is below the periformis.
Important clinical facts about the gluteal artery:
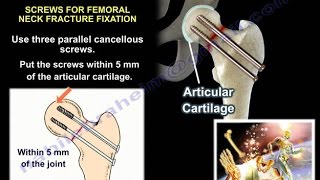
1 Harvesting bone graft from the posterior iliac crest: avoid going into the sciatic notch and injuring the superior gluteal artery.
2 Fracture of the acetabulum: extensile approach which is an extended iliofemoral approach, in this approach they dissect the entire gluteal muscle from the iliac crest from front to back and top to bottom, done until the posterior superior iliac spine and the greater sciatic notch, so the entire outer surface of the ilium is exposed, the entire gluteal muscle mass will be hanging by the superior gluteal artery, if you are going to take that approach, take care to protect that artery.
There is some concern with embolization of the superior gluteal artery or if fracture is going towards the greater sciatic notch.
3 Pelvic fractures: this artery is an important in pelvic fractures, people die from pelvic fractures from hemorrhage, most of the hemorrhage is venous bleeding and fracture bleeding, but some cases (about 10%) die from arterial bleeding.
The highest mortality of these patients usually occurs on patients that have shock on presentation to the emergency room; these are the people that require massive blood transfusion, so the more the hemorrhage the more the mortality.
CT angiography may be helpful in determining if any arterial injury is preset.
The criteria for angiography and embolization is not well established, but if the patient continue to be unstable, despite giving blood, let’s say 4 units of blood in the first hour, then you will probably need angiography and embolization.
What if the artery is injured during surgery?
It could retract into the pelvis, when you find it you clip it, and make sure you don’t clip the superior gluteal nerve.
Make sure anesthesia have enough blood available.
Make sure you tell everybody that you have a major arterial bleed.
Ask for help.
Become a friend on facebook:
/ drebraheim
Follow me on twitter:
https://twitter.com/#!/DrEbraheim_UTMC
Donate to the University of Toledo Foundation Department of Orthopaedic Surgery Endowed Chair Fund:
https://www.utfoundation.org/foundati...