Von Gierke (Glycogen Storage Disease 1) for USMLE
Von Gierke which is Glycogen Storage Disease Type 1 for Medical Students and USMLE. Covering Pathophysiology, Sign, Symptoms, Clinical Findings as well as Treatment Diagnosis and Management of the condition.
PATHOPHYSIOLOGY
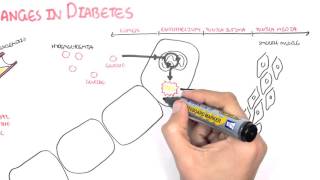
Glucose 6 phosphate attaches phosphate to Glucose to prevent loss of Glucose after entering the cell. The Glucose 6 phosphate goes into the cell through the transporter Glucose 6 phosphate Transporter 1. This Glucose 6 phosphate goes into the ER through the transporter. Then it comes into contact with glucose 6 phosphatase which is bound on the inside of the endoplasmic Reticulum. The Glucose 6 phosphate will be transformed into glucose and inroganic phosphate. Then there are glucose transporter which allows glucose to leave transporter into cytosol and then it can leave. Glucose 6 phosphate can also come from glycogen which is a chain of glucose. When it breaks down it becomes glucose6phosphate.
In Von Gierke Disease 1a there is a deficiency of Glucose 6 phosphatase enzyme and Von Gierke 1b there is a deficiency of glucose6 phosphate transporter 1 (G6PT1)
When there is overload of Glucose6Phosphate it goes into alternative pathways. It can go to the Pentose Phosphate Pathway to make Ribose5Phosphate. Therefore cataboli process gets activated and becomes uric acid, therefore patient can have hyperuricemia and predispose to gout. Since it can't make glucose from glycogen there is fasting hypoglycemia. There will also be increase pyruvate which will be converted to lactic acid which leads to lactic acidosis. Pyruvate is also a substrate for alanine so there is hyperalanemia. Acetyl CoA will also be overwhelmed and begin making more cholesterol and Fatty Acid which bind with glycerol to form Triacyl glycerol causing hyperlipidemia. So in summary there is hypoglycemia, hyperuricemia, hyperlaanemia, lactic acidosis, hyperhcoelsterolemia and hypertriglyceridemia.
Signs symptoms and clinical findings.
In neonatal period there is hypoglycemia which can predispose to seizures. There will be lactic acidosis and hyperuricemia. After 34 months there is a condition called "doll face" which fat cheeks, large arms. Distended abdomen may also be present due to hepatomegaly, enlarged kidney and even may get hypotonia. Long Term can lead to hepatic adenoma which can lead to hemorrhage. Increase cholesterol leads to production of increased hormones and even lead to PCOS without the hirsutism and acne. Pulmonary hypertension, pancreatitis form the hyperlipidemia. There may also be renal problems, usually after 20 years. Proteinuria may be seen. Hypertension and kidney stones may also be there and eventually dialysis and transplant of the kidney and liver is required.
DIAGNOSIS
Generally it is a clinical diagnosis. Lab work will show low glucose with high lipids, high uric acid, high lactate and high alanine. Definitive will require liver biopsy and look for the mutation.
TREATMENT
If you can maintain blood glucose level will help avoid many fo the problems. Thi ccan be done by feeding through NG tube or TPN. Uncooked corn starch has been the most successful because of slow absorption of glucose. Decrease uric acid through allopurinal, xanthine oxidase inhibitor. Treat lipidemia thorugh HMGCoA reductase inhibitors. ACE Inhibitors help protect the kidneys. Neutropenia