wrist fractures symptoms examination diagnosis and treatment.
Dr. Ebraheim’s educational animated video describes the common types of distal radius wrist fracture. Fractures distal radius symptoms, diagnosis, examination and treatment
The most common types of the distal radius fractures:
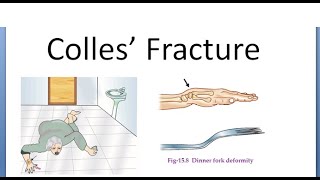
Colles fracture:
• the most common type,
• It is a distal radius fracture in the wrist, has a characteristic backwards displacement of the hand.
• It’s a low energy fracture, extra articular fracture with dorsal displacement of the distal fracture fragment.
• It typically occurs in patients more than 50 years old from attempting to break a fall with an outstretched hand.
• This fracture some times is referred to as “dinner fork” deformity, due to the shape of the fractured forearm.
• TFCC tears occurs in 50% of extraarticular distal radius fractures versus 1/3 of intra articular fractures.
• Dorsal comminution is frequent and if comminution is to 50% of the dorsal cortex, then treatment with a cast will not work. The more dorsal flexion, then the more comminution and more chance of fracture failure when using a cast.
• Colles fracture that extends to the DRUJ has a worse prognosis.
Smith fracture:
• Is an extra articular transverse fracture that is displaced in a volar direction and can be thought of as a reverse Colles fracture.
• It could occur from a fall onto a flexed wrist.
• This fracture has multiple types:
1 Type I: fracture is extra articular transverse fracture through the distal radius (most common)
2 Type II: fracture crosses into the dorsal articular surface.
3 Type III: fracture enters the radiocarpal joint (volar barton fracture equals a Smith type III fracture), both will involve the intra articular distal radius and includes possible dissociation of the carpal bones.
Die Punch fracture:
• Is a depressed fracture of the lunate fossa that results from axial loading forces on the distal radius that is transmitted through the lunate bone.
• It is intra articular fractures of the lunate fossa of the distal radius.
• Check to see if there is any carpal bone dissociation.
Bartons fracture:
• Intra articular fracture of the distal radius with dislocation of the radiocarpal joint.
• These fractures can be dorsal or volar.
• Check for carpal bone disruption or dissociation.
• It is caused by a fall on an extended and pronated wrist with the volar type being the most common type. The fracture fragment is usually smaller with the dorsal barton fracture.
• The volar barton fracture is the fracture of the volar margin of the of the distal radius, which is associated with subluxation of the radiocarpal joint.
• The most striking finding is subluxation or dislocation of the wrist with that small fragment.
• You can see in the picture the strong volar radiocarpal ligament avulses the volar lip of the radius.
• This fracture is very similar to the Smith type III fracture.
• Treatment of volar barton fracture is usually surgery with a volar approach and volar plate.
• Dorsal Barton: the dorsal shearing force, distal radius fracture with dislocation of the radiocarpal joint, fracture is intraarticular and involves the dorsal lip.
Dislocation is the most striking xray finding. The avulsed fragment is usually small.
Treatment is open reduction internal fixation through a dorsal approach.
Chauffer fracture:
• Is fracture of the radial styloid process in association with scapholunate dissociation.
• It is caused by compression of the scaphoid bone of the hand against the styloid process of the distal radius.
• Evaluation of the radial styloid fracture should always include supinated view xrays so that scapholunate dissociation can be ruled out.
• Look for major swelling of the wrist and distal DISI deformity on lateral xrays with a widening gap between the lunate and scaphoid bones on AP view.
• DISI deformity: the scapholunate angle is usually about 47° and can be up to 60°, any angle that is greater than 60° is considered abnormal; this is usually seen with a DISI deformity due to the palmar flexion of the scaphoid. This means that there is scaphoid dissociation. The scaphoid and lunate bones turn in opposite directions.
• Treatment of this fracture is: compression screw fixation of the radial styloid process.
• Assess the scapholunate joint for possible stabilization.
In conclusion:
During assessment of the xrays, you need to see if there is any involvement of the dorsal or volar rim of the radius.
Check for involvement of the DRUJ and look for diepunch lesions.
Check for dislocation of the wrist and the direction of the displacement.
Check the carpal distribution to see if there is any dissociation between the carpal bones
special thanks for NATHAN ELKINS FOR HIS CONTRIBUTION TO THIS VIDEO